Global Journal of Rare Diseases
Double homozygous Cystic Fibrosis Transmembrane Regulator gene (CFTR) mutation: A case series and review of the literature
1Department of Pediatrics, King Faisal Specialist Hospital and Research Centre (KFSHRC), Riyadh, Saudi Arabia
2College of Medicine, Sulaiman Al Rajhi University, Qassim, Saudi Arabia
3University at Buffalo- Catholic Health, Buffalo, New York, USA
4Elm University for Dentistry and Pharmacy, Riyadh, KSA, Saudi Arabia v
5Department of Genetics, Research Center, (KFSHRC), Riyadh, Saudi Arabia
Author and article information
Cite this as
Banjar H, Alkassas W, Ghomraoui F, Ghomraoui R, Moghrabi N (2020) Double homozygous Cystic Fibrosis Transmembrane Regulator gene (CFTR) mutation: A case series and review of the literature. Glob J Rare Dis. 2020; 5(1): 15-21. Available from: 10.17352/2640-7876.000023
Copyright License
© 2020 Banjar H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Introduction: Double homozygous mutation with the presence of double mutations in each allele is a very rare phenomenon with only 2 reports that have described this phenomenon in the medical literature.
Objective: To find the prevalence of double homozygous in our Cf population and to describe their mutations and review of the literature in this phenomenon.
Methodology: A case series and a review of the literature from 1989-2020 for similar phenomenon.
Results: A total of 396 patients (312 families) confirmed CF that were positive for the cystic fibrosis transmembrane conductance regulator (CFTR) variants from January 1998 to December 2018. A total of four families that constitute 4 patients were positive for double homozygous CFTR mutations in Trans position status. All parents were first-degree cousins. Their clinical pictures were of the severe type in relation to chest disease and failure to thrive. Family screening showed that 7 family members were carriers with double heterozygous mutations in Cis position. The Prevalence of double homozygous CFTR mutation in our study is 4/312 families or 1-2:100 families which is the highest that has been reported in the medical literature. Literature review showed only 2 cases of double homozygous were reported in 1995 and 2017.
Conclusion: Double homozygous CFTR mutations are common in the Saudi population due to consanguinity. Proper and extended genetic counseling is needed for the same family and their relatives to prevent similar conditions.
Cystic Fibrosis (CF) is an autosomal recessive disease and is considered the most common lethal disease of this category in Caucasians. In United Kingdom, its incidence is ∼1 in 2500-3000 among the Caucasian population with a mean prevalence of 0.737\10000 in European Union [1,2].
Approximately 2000 known variants have been identified for the CF gene [3]. Six different classes of variants are described depending on the fate of the protein coded by the cystic fibrosis transmembrane conductance regulator (CFTR) gene. Mutations in the gene lead to altered protein synthesis, which leads to insufficient active CFTR at the cell surface that affect the chloride ion channel function lead to dysregulation of epithelial fluid transport in the lung, pancreas and other organs, resulting in cystic fibrosis. Mutations consist of replacements, duplications, deletions or shortenings in the CFTR gene [4]. This may result in proteins that may not function, work less effectively, are more quickly degraded, or are present in inadequate numbers [3,4].
Several studies about CF showed that chest infection, steatorrhea, failure to thrive and Pseudo-Barrter’s Syndrome are the main clinical presentations [5,6]. In other Gulf countries, CF populations shared common disease traits [7,8].
CF population in Saudi Arabia has poor compliance with chest physiotherapy and medication, poor nutrition and early colonization of bacteria [5,6]. Around 50% of CF patients had colonization with Pseudomonas Aeruginosa at a mean age of 34 months [3], and this is significantly earlier than the age reported in Europe, where the mean age for colonization in these studies is 5 - 7 years of age [1,2].
It is reported that there are more widely-varied differences in Cystic Fibrosis transmembrane conductance Regulator gene mutations (CFTR) in the Saudi population than in other populations [6,9]. This can be due to consanguineous marriages that were reported to be 80% compared to the general Saudi population of 50%, which maintained the existence of these mutations [9]. The importance of identification of the CF-causing mutations is to provide genetic counseling, studying phenotype/ genotype correlation, family index and cascade testing of its carriers. Promisingly, identification of mutation type helps in targeting the best treatment for CF patient and to develop specific treatment for each case [10].
In the United Kingdom, 56 different types of CFTR mutations that account for 86% of CF genes were reported [11].
Double homozygous CFTR, is a very rare phenomenon with the presence of double mutations in each allele in transposition, and has been only described twice in the medical literature since the description of the CFTR mutation in 1989 [12,13]. One of these cases were describe in 1995 as part of complex CFTR mutation [12], and the other case was described by the current author from the same center [13].
The aim of our study is to find the prevalence of double homozygous in our Cf population and describe our (CFTR) mutations and their clinical picture, their family screening, and literature review of this phenomenon since the discovery of the CFTR mutation in 1989.
Methodology
This study is a retrospective case series study performed through reviewing all referred CF patients to our clinics in a tertiary-care center in Saudi Arabia from 1998 to the end of 2018. The diagnosis of CF was based on a typical clinical picture of cough, sputum production, and two subsequent samples of high sweat chloride levels (>60 mmol\L) by the Wescor quantitative method [5].
Respiratory cultures were taken from nasopharyngeal aspirates for patients younger than 5 year of age; and from induced sputum for patients older than 5 years of age. Cultures of broncho-alveolar lavage specimens were taken from 10% percent of the encountered CF population. Pancreatic insufficiency was diagnosed based on stool elastase measurements of > 100–200 ug/g, or a 72-hour fecal fat estimation using the van de Kamer method [12] of which a positive result corresponded to a fecal fat content >7 g/24 hours. Bronchiectasis was identified as dilated bronchi through radiological studies like chest X-rays or Computed Tomography (CT) scans [12].
Definition of CFTR genotype
A detailed family history was taken and screening to identify other family members affected with CF was performed. A homozygous genotype was identified as identical homozygous pathogenic CFTR variants. Compound heterozygous mutations were identified as two different pathogenic CFTR variants occurred in a trans configurations at two different alleles for the same chromosome. In a heterozygous genotype, one variant was identified in one allele [9].
In double homozygous genotype, two different CFTR pathogenic variants in one chromosome with a carbon copy of the same variant in trans position location in the other allele [9].
CFTR allele counts for patients and families
Multiple siblings with a homozygous CFTR variant within the same family are counted as having two alleles. In a compound heterozygous CFTR variant, each variant is counted as one mutant allele separately (i.e., multiple CF-affected siblings within the same family will be counted with each CFTR variant separately). The percentage of alleles for the patients is calculated as the number of affected alleles for a certain CFTR variant divided by the total number of alleles for the whole CF population (396 patients/792 alleles). The percentage of alleles for the families is calculated as the number of families with the affected alleles for a certain CFTR variant divided by the total number of alleles for whole CF population (312 families) [9].
CFTR identification
The CFTR gene screening methodology involves DNA isolation, Polymerase Chain Reaction (PCR) amplification of genomic DNA, mutational analysis, and sequencing methods [14]. Genomic DNA from the patient’s lymphocytes was used to amplify the 27 exons and flanking sequences of the CFTR (NM_000492.3; NP_000483.3). The PCR products were analyzed by sequencing in both the forward and reverse directions and were applied according to currently recommended methods [15,16]. Variant detection was scored using publicly available variant databases for CF such as the Cystic Fibrosis Mutation Database (http://www.genet. sickkids.on.ca/CFTR/Home.html) and The Human Gene Mutation Database - Professional Edition (http:/www.hgmd.cf.ac.uk/ac/index.php). Both mutation databases provided an extensive repertoire of up-to-date sequence variants, deletions and insertions for the CFTR gene.
The screening included all 1st degree relatives, brothers, sisters (Healthy and symptomatic siblings) and parents. Others relatives are screened on the request of the family.
Ion torrent as the next generation sequencing [17]
Ion Torrent semiconductor technology is a recent comer as Next Generation Sequencing Platform that is currently already being adopted at top medical institutions worldwide such as Baylor College of Medicine, USA. Our facility is currently equipped with 12 Ion Torrent PGM (Personal Genome Machines), and 2 Ion Protons for use in both research and molecular diagnostics of genetic disorders. It is based on scoring fluctuations in pH upon the natural release of a proton occurring spontaneously upon DNA polymerization. At the core of the technology is a semiconductor chip that comprises a high-density array of micro-machined wells where simple biochemical process of DNA polymerization takes place and in a massively parallel way. Each well holds a single bead with attached single strand template DNA to be sequenced, and with each bead having multiple such copies of identical template DNA. Beneath each well is a proton sensitive layer, and beneath that layer is a proprietary proton sensor; thus each well in an Ion Torrent chip is effectively a solid-state pH micro-meter. This method is used in some of our patients recently.
Ethical consideration
After obtaining ethical approval by the Research Advisory Committee. (IRB) project number 21110 16, and dated 11th March 2015 and the Declaration of Helsinki, good clinical practice guidelines were followed. Data collection and data entry were supervised by the principal investigator. All data were obtained by retrospective chart review and were stored in the Pediatrics Research Unit, accessed only by the principal investigator and the assigned clinical research coordinator. Patients’ information was kept strictly confidential. Each patient was given a study number, and all patient data were entered into the designed data sheet without patient identification.
Results
From January 1998 to December 2018 and among 396 patients (312 families) had been confirmed of having CF were positive for CFTR variants. A total of 4 families that constitute 4 patients with confirmed CF were positive for double homozygous CFTR mutations in trans position location. All parents were first degree cousins. Their clinical pictures were of the severe type in relation to chest disease, failure to thrive, progressive bronchiectasis, worse Pulmonary function test parameters, persistent vitamins ADEK deficiencies compared to the rest of the CF population. Two out of 4 patients had Methicillin-resistant Staphylococcus aureus (MRSA) compared to 6% of our CF population (author’s own data).
Family screening found 7 family members were carriers with double heterozygous state in cis position (in the same allele) with normal sweat chloride test and normal growth. The range age of diagnosis is between 3 to 12 months of age [Table 1] [18-21].
| Table 1: Double Homozygous CFTR mutations, Patients’ Clinical Data (Total of 4 families). | ||||
| Variable | Patient 1 HN | Patient 2 ZB | Patient 3 AF | Patient 4 LN |
| Age at Presentation | 3 m | 12 m | 5 m | 5 m |
| Age at FU | 4 Y | 10 Y | 4 Y | 7 Y |
| Province (KSA) | Qunfutha/ West |
Dammam/ East |
Madinah Almunawarah/ West |
Riyadh/ Central |
| S/S | - PI - Intestinal obs - MI |
- Pulm atelectasis - Mild fatty liver - Cholestasis - CHD |
- Bronchiectasis - Atelectasis |
- Fatty liver bronchiectasis |
| CFTR | - c.1399C>T; Exon 1118 - c.1521_1523delCTT; Exon 1119 |
-c.3889dupT; Exon 2420 -c.1521_1523delCTT; Exon 1119 |
- c.343G>T; Exon 421 - c.3100C>T; Exon 19 |
- c.1399C>T; Exon 1118 c.1521_1523delCTT; Exon 11 19 |
| CFTR (rs) | -rs1800089 -rs113993960 |
-rs121908808 -rs113993960 |
-Novel mutation - rs1554392043 |
-rs1800089 -rs113993960 |
| PFT: | N/A | FVC=78%, FEV1= 85%, FEV1/FVC=95. MMEF=104%, FRC= 271%, RV=472, TLC=152 %, RV/TLC=64/288. | N/A | FVC=51%, FEV1=45%, FEV1\FVC= 89% |
| ALT, AST (1st) | 16, 28.5 U/L | 49, 49 U/L | 64, 50.4 U/L | 89, 92 |
| ALT, AST (FU) | 22.2, 30 U/L | 20.2, 19.3 U/L | 11.3, 22.3 U/L | 21.5, 33.9 |
| Sweat Cl | 72 mmol\L | 107 mmol\L | 105 mmol\L | 96 mmol\L |
| Bacterial Culture | MRSA Sterpt P= H-flue P aeruginosa |
Staph aureus Sterpt P= H-flue Moraxella catarrhalis. |
MRSA Staph aureus |
Moraxella catarrhalis P aeruginosa |
| Viral PCR | Entero Boca Influenza A Influenza B Metapneumo Rhino-viruses |
Para-flue Influenza Rhino C Boca Adeno Boca |
- Rhino | - Adeno |
| Vit A,D, E (1st) Mcg/L | 95, 13 , 2.2 | 185, 19, 2.7 | 394, 55, 12.5, Mcg/L | 134, 66, 11 |
| Vit A,D,E (FU) Mcg/L | 301, 54, 5.2 | 440, 36.2, 9 | 119, 109, 11.2 | 126, 47.4, 8.9, |
| Family Screening | - A sister is a carrier of two heteroz CFTR in c.I399C>T; Exon 11 and c.1521_1523deiCTT | - A brother is a carrier heteroz CFTR in cis c.164+12T>C; Intron 2 and c.3889dupT; Exon 24 - Another brother NM_000492; Exon24: c.3884du Heteroz - Two parents are carrier similar to his brother - An aunt is a carrier |
- A brother is a carrier of double heteroz CFTR in cis c.343G>T; Exon 4 and c.3100C>T; Exon 19 - A sister is a carrier of double heteroz mutations in cis c.343G>T; Exon 4 and c.3100C>T; Exon 19 |
Reported Mutations in Chromosomes |  |
| CFTR: Cystic fibrosis transmembrane conductance regulator; M: Months; Y: Year; KSA: Kingdom of Saudi Arabia; S/S: Signs and Symptoms; PI: Pancreatic Insuuficiency; Intestinal obstruction: Intestinal obs; MI: Meconium Ileus; CHD: Congenital Heart Disease; Novel Mutatio: Newly Described by our team Rs= refSNP: Reference Single Nucleotide Polymorphism Database; https://www.ncbi.nlm.nih.gov/snp/ PFT: Pulmonary Function Tests; FVC: Forced Vital Capacity; FEV1: Forced Expiratory Volume in 1st second; FEV1/FVC: Ratio of FEV1 to FVC; MMEF: Maximal Mid-Expiratory Flow; FRC: Functional Residual Capacity; RV: Residual Volume; TLC: Total Lung Capacity; N/A: Not applicable; ALT: Alanine Transaminase; AST: Aspartate Transaminase; FU: Follow-Up; Sweat cl: Sweat Chloride Test; MRSA: Methicillin-Resistant Staphylococcus Aureus; Sterpt P= Streptococcus Pneumoniae; H-flue: Haemophilus Influenzae; P aeruginosa: Pseudomonas Aeruginosa; Staph aureus: Staphylococcus Aureus; PCR: Polymerase Chain Reaction; Entero: Entero Virus; Boca: Human Bocavirus; Influenza: Influenza Virus; Metapneumo: Human Metapneumovirus; Rhino: Human Rhino Virus; Para-Flue: Para-Influenza Virus; Adeno: Human Adenoviruses; Vit: Vitamins |
||||
The Prevalence of double homozygous CFTR mutation in our study is 4/312 families or 1-2:100 families which is the highest that has been reported in the medical literature.
Discussion
Since the discovery of the CFTR gene in 1989, around 2000 CFTR mutations have been described [11,3]. A review of the literature showed several studies reported a combination of several complex CFTR mutations with 3-4 mutations in transposition location in both alleles (Table 2) [12,13,22-35].
Only one study described the double homozygous mutation as part of a complex CFTR description of their CF population [13], and the other 4 cases are from our CF population (Table 2).
| Table 2: Literature review of Complex CFR mutations (1989-2020) £. | ||
| Ref # |
Reported Mutations | Comment |
| 12 | 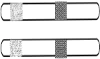 |
A case report of double homozygous of c.164+12T>C (IVS2+12T>C) in intron 2, and a second homozygous c.3889_3890insT (p.S1297FfsX5) in exon 24 in transposition configuration. Family screening of a healthy brother showed one copy of c.164+12T>C, in intron 2 (IVS2+12T>C) and c.3889dupT (c.3889_3890insT) in exon 24 (p.S1297FfsX5) in Cis configuration. CFTR analysis of both parents showed that they were both carriers for both mutations in exactly the same manner as the brother. |
| 13 | 
 double homozygous |
Reported 2 patients with complex mutations [G1069R + L88X allele and AF508], one patient with [S912L+G1244V and G542X] and one with double homozygous mutation of [G1069R + L88X] |
| 22 | 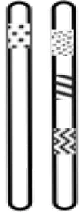 |
A case associated with a complex CFTR allele in 2 brothers. In the younger boy sweat test chloride showed a slightly increased chloride concentration (35 mEq/l); however, the test was not performed for the older sibling. Complex CFTR mutation carry three missense mutations from mother, D443Y (1459G>T, exon 9), G576A (1859G>C, exon 12), and R668C (2134C>T, exon 13), and N1303 from father. |
| 23 | 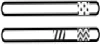 |
Novel complex heterozygous complex allele of [H939R; H949L] + R248T or G542X 1259insA or G1349D or F508del Allele. The mutations G542X, 1259insA, G1349D, |
| 24 |  |
Two mild CF-associated mutations result in severe cystic fibrosis when combined in cis and reveal a residue important for CFTR processing and function. R347H and D979A in Cis |
| 25 | 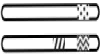 |
Severe cystic fibrosis associated with a F508 del/R347H+D979A compound heterozygous genotype. Sweat chloride test was 96 for one of them and 102 mEq\l for the other Complex of three mutation A F508del and R347H+D979A from mother |
| 26 |  |
Both patients with the complex allele F508C-Sl251N are carrying AF508 on the other CF chromosome. |
| 27 |  |
A case with A F508deletion-R553Q/R553 CFTR mutation. Borderline sweat test values were associated with typical clinical symptoms of CF. The patient was diagnosed to have CF at the age of 61~ y. |
| 28 |  Twins Twins
 Father Father |
The triple mutant p. [R74W; V201M; D1270N] allele associated with the unknown p.P841R mutations were detected in a father with congenital bilateral absence of the vas deferens. His twins are carrier for p.[R74W;V201M;D1270N] and have F508 from their mother |
| 29 |  |
Segregation analysis showed the father to be a carrier of 711+1G>T, and the mother of a complex allele [R74W;R1070W;D1270N] (HGVS: c.[220C>T; 3208C>T; 3808G>A]), confirming the patient as a compound heterozygote. |
| 30 |  |
R334W- R1158X\delF508 genotype. |
| 31 |  |
Reported 4 cases: 2 with W1282X/[R117L; L997F], one case of G85E/[R117L; L997F], and a case with F508del/[R117L; L997F] |
| 32 |  |
Several cases of complex CFTR alleles observed in a series of 157 patient samples after extensive sequencing (e.g. p.R1158X/[p.V562I;p.A1006E] DF508/[p.R352W;p.P750L] ) |
| 33 |  |
4 cases reported complex of three mutations as p.[Val754Met;CFTRdele3_10, 14b_16] with one different mutation in the other allele as following 1812-1G>A,3659delC,p.Asn1303Lys, and p.Phe508del |
| 34 |  |
7 patients have the complex allele 3199del6 + I148T with triple mutation of F508 in 5 patients, N1303K in one patient and Q890X in another patient. all 7 patients with a classic CF phenotype. |
| 35 |  |
An individual with the CFTR genotype R553X/F508del-R553Q showed the typical symptoms and electrophysiological anomalies of cystic fibrosis in the airways and intestine |
| £: mutations are mentioned in legacy names as written in the paper; Cis locations= same allele, Transposition= Different Allele | ||
Out of 312 screened families, four cases in four different families had both mutations in the two alleles in an identical way and were diagnosed as double homozygous mutations. Therefore, the prevalence of this genotype is accounted as 1.3% out of all reported cases. Such conditions may be due to the consanguinity between relatives in Gulf Arab communities that can be between two or more consecutive generations. Repetition of consanguinity will pool the present mutations in the affected family. More regulations and precautions should be taken to prevent such extremely rare phenomena. Family counseling and educational campaigns to increase the awareness about the risk of these marriages would help to decrease the inheritance of these mutations. For this reason, the presence of four cases indicates that it is relatively common in the Gulf Arab communities and we suggest more research to be done on the prevalence and distribution of this phenomena.
The clinical pictures were of the severe type in relation to chest disease, failure to thrive, progressive bronchiectasis, worse Pulmonary function test parameters, persistent vitamins ADEK deficiencies compared to the rest of the CF population, more frequent (MRSA) colonization compared to the general CF population.
Reporting the phenotype of this newly discovered genetic phenomenon will help in comparing it to other common and rare CF conditions and for studying the contributions of these mutations to the course of the disease. Moreover, it would help in individualized therapy and planning of the management [10] Family counseling and screening before marriage, and educational public campaigns might reduce or eliminate this extremely rare conditions that combine double identical mutations in one individual.
We believe identification of double homozygous mutations could help in personalized medicine and finding pharmacological treatment in the future such as Orkambi®(lumacaftor/ivacaftor) and Symdeko (Tezacaftor/Ivacaftor) from vertex for F508del mutation [36,37] and Ivacaftor (Kalydeco) for patients with G551D mutations and some other mutations [38].
Our study has limitation due to small number 4 cases. Further study is needed to do extensive family screening of the relatives of such families to understand the effect of such phenomenon.
Conclusion
Double homozygous CF is relatively common in Saudi Arabia and might be present in the other Arab Gulf countries due to having similar societies and consanguinity among their families. More public awareness is needed in these countries and similar communities to prevent such phenomena. It is important to report these newly discovered genotypes for personalized medicine of CF patients.
(1) Sara Alkaf, from Biostatistics, Epidemiology, and scientific computing Department, King Specialist Hospital and Research Center (KFSHRC), Riyadh. KSA for her contribution in data entry.
(2) Sami AlHaider. MD. for providing one patients.
- Hall BD, Simpkiss MJ (1968) Incidence of fibrocystic disease in Wessex. J Med Genet 5: 262-265. Link: https://bit.ly/2Y7T2xF
- Farrell PM (2008) The prevalence of cystic fibrosis in the European Union. J Cyst Fibros 7: 450-453. Link: https://bit.ly/315XaAk
- Banjar H., Angyalosi G (2015) The road for survival improvement of cystic fibrosis patients in Arab countries. Int J Pediatr Adolesc Med 2: 47-58. Link: https://bit.ly/3452p5g
- de Gracia J, Mata F, Alvarez A, Casals T, Gatner S, et al. (2005) Genotype-phenotype correlation for pulmonary function in cystic fibrosis. Thorax 60: 558-563. Link: https://bit.ly/31aI0Kl
- Banjar H (1999) Overview of cystic fibrosis patients aged 1-12 years in a tertiary care centre in Saudi Arabia. MIDDLE EAST Paediatr 4: 44-50.
- Kambouris M, Banjar H, Moggari I, Nazer H, Al-Hamed M, et al. (2000) Identification of novel mutations in Arabs with cystic fibrosis and their impact on the cystic fibrosis transmembrane regulator mutation detection rate in Arab populations. Eur J Pediatr 159: 303-309. Link: https://bit.ly/348Jpmh
- Dawson KP, Frossard PM (1995) Cystic Fibrosis in the United Arab Emirates: An Under-Recognized Condition? Trop Doct 25: 110-111. Link: https://bit.ly/3g7knqf
- Abdul Wahab A, Dawod ST, Al Thani G (2000) Cystic fibrosis in a large kindred family in Qatar. Ann Trop Paediatr 20: 203-207. Link: https://bit.ly/2DW0iWS
- Banjar HH, Tuleimat L, El Seoudi AA, Mogarri I, Alhaider S, et al. (2019) Genotype patterns of cystic fibrosis transmembrane conductance regulator gene muta¬tions: a retrospective descriptive study in Saudi Arabia. Ann Saudi Med 40: 15-24. Link: https://bit.ly/326e6G2
- Marson FAL, Bertuzzo CS, Ribeiro JD (2017) Personalized or Precision Medicine? The Example of Cystic Fibrosis. Front Pharmacol 8: 390. Link: https://bit.ly/2PZYJt5
- Schwarz MJ, Malone GM, Haworth A, Cheadle JP, Gardner A, et al. (1995) Cystic fibrosis mutation analysis: report from 22 UK regional genetics laboratories. Hum Mutat 6: 326-333. Link: https://bit.ly/2Q2LesJ
- Banjar H, Moghrabi N, Alotaibi T, Alotaibi S, Gamalmaz H (2017) The first case report of double homozygous of 2 different mutations in the CFTR gene in Saudi Arabia. Int J Pediatr Adolesc Med 4: 41-46. Link: https://bit.ly/3h7aVUN
- Savov A, Angelicheva D, Balassopoulou A, Jordanova A, Noussia-Arvanltakis S, et al. (1995) Double mutant alleles: are they rare? Hum Mol Genet 4: 1169-1171. Link: https://bit.ly/34aKQ3C
- Brunstein J (2013) PCR: the basics of the polymerase chain reaction. MLO Med Lab Obs 45: 34-35. Link: https://bit.ly/3h7X7cW
- Chatterjee N, Banerjee T, Datta S (2012) Accurate Estimation of Nucleic Acids by Amplification Efficiency Dependent PCR. PLOS ONE 7: e42063. Link: https://bit.ly/3azXwm3
- Gomes C, Martinez-Puchol S, Pons MJ, Bazán J, Tinco C, et al. (2016) Evaluation of PCR Approaches for Detection of Bartonella bacilliformis in Blood Samples. PLoS Negl Trop Dis 10: e0004529. Link: https://bit.ly/3hkipnT
- Goldfeder RL, Wall DP, Khoury MJ, Ioannidis JPA, Ashley EA (2017) Human Genome Sequencing at the Population Scale: A Primer on High-Throughput DNA Sequencing and Analysis. Am J Epidemiol 186: 1000-1009. Link: https://bit.ly/315UaE9
- Elahi E, Khodadad A, Kupershmidt I, Ghasemi F, Alinasab B, et al. (2006) A Haplotype Framework for Cystic Fibrosis Mutations in Iran. J Mol Diagn 8: 119-127. Link: https://bit.ly/34bgm1w
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, et al. (1989) Identification of the cystic fibrosis gene: Cloning and characterization of complementary DNA. Science 245: 1066-73. Link: https://bit.ly/2Ydlo9X
- Schrijver I, Ramalingam S, Sankaran R, Swanson S, Dunlop CL, et al. (2005) Diagnostic Testing by CFTR Gene Mutation Analysis in a Large Group of Hispanics: Novel Mutations and Assessment of a Population-Specific Mutation Spectrum. J Mol Diagn 7: 289-299. Link: https://bit.ly/3h79N3v
- Castellani C, Assael BM (2017) Cystic fibrosis: a clinical view. Cell Mol Life Sci 74: 129-140. Link: https://bit.ly/3iOpkWy
- Abramowicz MJ, Dessars B, Sevens C, Goossens M, Boulandet EG (2000) Fetal bowel hyperechogenicity may indicate mild atypical cystic fibrosis: a case associated with a complex CFTR allele. J Med Genet 37: e15-e15. Link: https://bit.ly/3hdpLti
- Polizzi A, Tesse R, Santostasi T, Diana A, Manca A, et al. (2011) Genotype-phenotype correlation in cystic fibrosis patients bearing [H939R; H949L] allele. Genet Mol Biol 34: 416-420. Link: https://bit.ly/3iPtLAn
- Clain J, Fritsch J, Lehmann-Che J, Bali M, Arous N, et al. (2001) Two Mild Cystic Fibrosis-associated Mutations Result in Severe Cystic Fibrosis When Combined in Cis and Reveal a Residue Important for Cystic Fibrosis Transmembrane Conductance Regulator Processing and Function. J Biol Chem 276: 9045-9049. Link: https://bit.ly/31aFDHr
- Hojo S, Fujita J, Miyawaki H, Obayashi Y, Takahara J, et al. (1998) Severe cystic fibrosis associated with a AF508/R347H + D979A compound heterozygous genotype. Clin Genet 53: 50-53. Link: https://bit.ly/2Y9c4DY
- Kälin N, Dörk T, Tümmler B (1992) A cystic fibrosis allele encoding missense mutations in both nucleotide binding folds of the cystic fibrosis transmembrane conductance regulator. Hum Mutat 1: 204-210. Link: https://bit.ly/313fl9R
- Dörk T, Wulbrand U, Richter T, Neumann T, Wolfes H, et al. (1991) Cystic fibrosis with three mutations in the cystic fibrosis transmembrane conductance regulator gene. Hum Genet 87: 441-446. Link: https://bit.ly/3g3Ote1
- Brugnon F, Bilan F, Heraud MC, Grizard G, Janny L, et al. (2008) Outcome of intracytoplasmic sperm injection for a couple in which the man is carrier of CFTR p. [R74W; V201M; D1270N] and p.P841R mutations and his spouse a heterozygous carrier of p.F508del mutation of the cystic fibrosis transmembrane conductance regulator gene. Fertil Steril 90: 2004.e23-2004.e26. Link: https://bit.ly/3iR6r5n
- de Prada Merino A, Bütschi FN, Bouchardy I, Beckmann JS, Morris MA, et al. (2010) [R74W;R1070W;D1270N]: A new complex allele responsible for cystic fibrosis. J Cyst Fibros 9: 447-449. Link: https://bit.ly/3iNy5QE
- Duarte Â, Amaral M, Barreto C, Pacheco P, Lavinha J (1996) Complex cystic fibrosis allele R334W-R1158X results in reduced levels of correctly processed mRNA in a pancreatic sufficient patient. Hum Mutat 8: 134-139. Link: https://bit.ly/3g4qxaA
- Lucarelli M, Narzi L, Pierandrei S, Bruno SM, Stamato A, et al. (2010) A new complex allele of the CFTR gene partially explains the variable phenotype of the L997F mutation. Genet Med 12: 548-555. Link: https://bit.ly/31Z4v3S
- McGinniss MJ, Chen C, Redman JB, Buller A, Quan F, et al. (2005) Extensive Sequencing of the CFTR gene: lessons learned from the first 157 patient samples. Hum Genet 118: 331-338. Link: https://bit.ly/2EceHxS
- Niel F, Legendre M, Bienvenu T, Bieth E, Lalau G, et al. (2006) A new large CFTR rearrangement illustrates the importance of searching for complex alleles. Hum Mutat 27: 716-717. Link: https://bit.ly/31Z4hK4
- Rohlfs EM, Zhou Z, Sugarman EA, Heim RA, Pace RG, et al. (2002) The I148T CFTR allele occurs on multiple haplotypes: A complex allele is associated with cystic fibrosis. Genet Med 4: 319-323. Link: https://bit.ly/3aANBwq
- Tümmler B, Stanke F, Bronsveld I, Veeze H, Ballmann M (2009) Transient correction of the basic defect in sweat glands in an individual with cystic fibrosis carrying the complex CFTR allele F508del-R553Q. Thorax 64: 179-180. Link: https://bit.ly/34buoAm
- Bear CE (2020) A Therapy for Most with Cystic Fibrosis. Cell 180: 211. Link: https://bit.ly/3aAQOvZ
- De Boeck K (2020) Cystic fibrosis in the year 2020: A disease with a new face. Acta Paediatr 109: 893-899. Link: https://bit.ly/2CFqhkG
- Whiting P, Al M, Burgers L, Westwood M, Ryder S, et al. (2014) Ivacaftor for the treatment of patients with cystic fibrosis and the G551D mutation: a systematic review and cost-effectiveness analysis. Health Technol Assess 18: 1-106. Link: https://bit.ly/3h8nBLc



 Save to Mendeley
Save to MendeleyArticle Alerts
Subscribe to our articles alerts and stay tuned.
 This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International License.

